Read the previous part of the article.
Read the full report.
We consider it appropriate to conduct a comprehensive criminological and psychobiographical analysis of the role of psychoactive substances in shaping Alexander Dvorkin’s behavioral trajectory. His practical knowledge of pharmacological properties of various psychoactive substances deserves particular attention, including their combinations, effects, overdose risks, and potentially lethal consequences.
Substance abuse is defined as non-medical intake of chemical substances that affect one’s central nervous system and mental functions. It further damages areas of the brain, leading to impulsivity, aggression, and antisocial behavior. This closely correlates with rising criminal aggression and crime.
A neuroimaging study on addiction (Goldstein & Volkow, 2011) 1, supported by the U.S. National Institute on Drug Abuse, shows that chronic intake of psychoactive substances and intoxication itself disrupt functioning of the prefrontal cortex in drug-addicted individuals. This lowers frustration tolerance, impairs impulse control and the ability to assess consequences, which intensifies aggression and antisocial behavior, and explains the impulsive and risky behavior of addicts.
Neuropsychiatric studies 2 also note that individuals with criminal behavior and violent offenses often show damage to the prefrontal cortex. When combined with addiction, the risk of aggression rises sharply.
In the context of criminal psychology, abuse of psychoactive substances is viewed as a concomitant factor that can lower the threshold of self-control, increase impulsivity and a propensity for risk-taking, alter values, and determine antisocial behavior, often leading to recidivism. Studies indicate that psychological deformations, aggressive behavior, and cognitive distortions serve as the primary psychological factor underlying the criminal behavior of a drug addict. Offenders exhibit similar patterns of thinking. Those include persistent lying, lack of self-criticism, inability to empathize, a drive for immediate gratification, and shifting blame onto other people and circumstances. In individuals predisposed to antisocial behavior (for example, those with pathological personality development or psychopathic traits), chronic substance abuse can exacerbate existing cognitive distortions, contributing to criminalization. Thus, drug addiction and psychoactive intoxication act as catalysts and amplifiers of latent deviant tendencies.
Despite Alexander Dvorkin’s public claims about his lack of knowledge of “physics and chemistry,” data from autobiographical and biographical sources indicate that Alexander Dvorkin possesses a detailed understanding of how psychotropic substances work. Not only does he know how to induce certain mental states with their help, but he also knows how to combine them with medications to enhance or modulate their effect, even to the point of creating potentially life-threatening combinations.
This level of competence is explained by a combination of factors:
1. Family environment: His grandfather, who largely replaced his absent father, served a sentence for crimes related to “chemistry” (“my grandfather served a considerable sentence in a Stalin’s labor camp,” “he served his term for chemistry.”), which suggests the presence of specific information in the family environment where Dvorkin grew up.
2. Immediate relatives: Alexander Dvorkin’s sister was raised in the family and registered with a psychoneurological clinic, suggesting Dvorkin had access to psychotropic medications at home and observed their effects.
3. Personal experience as a patient: Dvorkin himself spent several years under the supervision of specialists at a psychoneurological clinic and underwent inpatient treatment in a psychiatric hospital where he acquired practical knowledge of dosages, mechanisms of action, and side effects of psychopharmacological agents.
4. Professional episode in the medical field: While registered with a psychoneurological clinic, Alexander Dvorkin briefly worked as an orderly in a trauma intensive care unit where he had access to psychoactive substances.
5. Long-term experience using psychoactive substances: As a person with a long history of psychoactive substance use, Dvorkin acquired experience and knowledge, including an understanding of psychopharmacological agents, their various combinations, dosages, methods of manufacturing narcotic substances, as well as skills in managing psychoactive states — achieving targeted alterations of consciousness and recognizing risks associated with overdose and lethal combinations of substances.
Thus, Alexander Dvorkin’s knowledge of psychopharmacology goes far beyond everyday experience and approaches a practical, albeit informal, competence. This makes him potentially capable of deliberately using psychoactive substances as a tool of influence, including for criminal purposes. Information from the examined autobiographical, biographical, and other open sources contains a significant number of episodes with content indicating the role of psychoactive substances in shaping Dvorkin’s behavioral trajectory, his practical knowledge of the pharmacological properties of various psychoactive substances, his substance use (polydrug use), and his interaction with social circles involved in the drug environment, both as consumers and as participants in their distribution.
This article provides only a few illustrative examples — excerpts taken from:
- Arkady Rovner’s novel “Kalalatsy” 3 (first published in 1980) written based on Alexander Dvorkin’s oral accounts;
- A 1979 interview given by Alexander Dvorkin for the project “Recent Soviet Immigrants in America” 4;
- Alexander Dvorkin’s autobiographical book “My America” (2013) 5.
Episode 1. “Hello, kids,” Lopukhov nodded, laughing, “My name is Jimi Hendrix. I’ve taken a dose of heroin; in five minutes it’ll start to take effect, but in the meantime, I’ll play something for you. To be honest, guys, I’m a scumbag, but I can play the guitar.” Then, switching back to his own voice, he said, “Allright, keep singing, Buptov. I like listening to you and then passing it off as my own. I’m considered a theoretician among my gang — thanks to you. You got any booze?” 3
Episode 2. “Usually they started with sleeping pills, some diphenhydramine — half a pack, a pack or two. I didn’t go through the diphenhydramine stage and was very proud of that: it gives you a heavy dullness. Diphenhydramine is an antiallergic drug with a sedative side effect. There was a funny story in Kyiv: a guy walked into a pharmacy and asked for diphenhydramine, and they told him, ‘We’ve run out of it. Hippies ate it all.’
“After diphenhydramine they started taking seduxen, eunoktin, noxiron, as well as all barbiturate-class sleeping pills: Barbamil, phenobarbital and others — in short, barbiturates. At this same stage they started smoking dope: hashish, hemp, anasha, marijuana resin — roughly sifted hashish (cannabis pollen) — and marijuana (ground leaves). The entire ‘old system’ went through the barbiturate stage and got stuck on seduxen.
“If a hospital gives you an antidepressant, it can cause severe convulsions, so you need cyclodol as a corrective. But if you take cyclodol on its own, you get vivid hallucinations. Noxiron, like seduxen, is eaten by the handful — five or more at a time. Then it stops putting you to sleep and starts working as intended.
“Once — I was already studying at the institute then — Alyona and I took a lot of seduxen and walked around in bliss. She stole five eggs from the cafeteria. I asked why, and she said, ‘Wait, you’ll see.’ When we went outside, she started throwing the eggs at the institute wall and, as she threw them, kept saying, ‘That’s why! that’s why!’” 3
Episode 3. “Anyone who went through the seduxen stage — if they went through it, because people got stuck at every stage — moved on to codeine with noxiron, and that was when the true meaning of noxiron revealed itself. If you take one noxiron for every five codeine pills, the high comes out beautiful and clean, like a Chinese engraving.
One day, someone played a cruel joke on me. Poppy season had ended, I hadn’t yet hustled up new injection sites, and the old ones had closed. So I went to a doctor I knew — he gave me fentopil. I shot it into my butt — I’d heard from someone that if you inject it into a muscle, you get a beautiful codeine-like high — and headed to Alyona’s birthday. Suddenly my back arched backward and my neck forward — my whole body twisted up.” 3
Episode 4. “Somewhere between seduxen, codeine, and cyclodol, people started sniffing — smoking weed continued at all levels. After passing the lower stages, a person switched into the ‘noble’ drugs, and all the rest were cut off. What remained was dope, opiates, and cocaine.
Opiates are codeine, morphine, fentopil, and, of course, homemade opium from poppies. (Fentopil is a Hungarian drug; it is given with droperidol before surgery so a patient doesn’t get anxious.) There are several technologies for producing homemade opium…” 3
These and other data indicate that the subject of our study practiced simultaneous use of multiple psychoactive substances (polysubstance addiction) and understood their potentially lethal consequences, including based on observing the fates of his acquaintances. It is known that in the late 1970s, a common combination among people using psychoactive substances was diazepam belonging to the benzodiazepine family (in the USSR, it was marketed under the trade name seduxen) and other central nervous system depressants, including alcohol and opioids (e.g., morphine). When diazepam (seduxen) is used with these substances, the depressive and sedative effects of both drugs intensify exponentially, sharply increasing the risk of overdose.
A simultaneous combination of diazepam and opioids causes dangerous side effects. According to pharmacological studies 6, the concurrent use of benzodiazepines and opioids leads to a synergistic amplification of their depressive effects: respiratory depression, lowered blood pressure, impaired consciousness, and a sharp increase in the risk of coma and death. Even at therapeutic doses, such a combination can cause deep sedation, cognitive impairment, disorientation, and a loss of sound judgment. In cases of overdose, the risk of death rises exponentially.
Episode 5.
“Existing from summer to the psychiatric hospital, and then again — from the psychiatric hospital to summer… Thank God, this affected me less so far, my friends much more, but in this alternation of periods of free life with psychiatric dungeons there was a fatal inevitability that came at a high price.”
Episode 6.
“In addition, there was yet another extremely important problem: drugs. Gradually they seeped into our environment and, like poison, contaminated it. I’m not talking about the inevitable disintegration of personality which they led to. They also corrupted our entire brotherhood. In fact, with the spread of drugs, it ceased to exist: only isolated loners remained, each interested solely in where to get the next dose. Over time, a dose began to replace all ideas, friends, love, and, eventually, life itself. We increasingly encountered dealing among ourselves, theft, betrayal of friends, and abandonment of the closest people. Arrests also became more frequent: authorities now had an absolutely impeccable pretext to fight us. Then we started seeing the first people among us dying from overdoses and other drug-related causes.”
Episode 7. Excerpts from Alexander Dvorkin’s interview [1979]:
“A: Well, just reaction of the authorities. When actually the Moscow hippie movement started one of the reasons was the Western hippies and they were just trying to do something like that, but it was taken very seriously from the authorities and then, I don’t know, it came out underground movement. It wasn’t me, but at one time it was really popular among the students, and at the time when I left it was down already, everybody had forgotten about them and the ones that were left were practically all heavy drug addicts and each of them had spent years in mental hospitals.”
Episode 8.
“Q. When you say hippie culture for the Soviet Union, are you using that to mean drug culture, or are you making a difference between the two?
А. Yes, I’m making a difference for it because hippie culture weren’t born on drugs, so… The drug culture appeared just much later, and it was very tightly tied together. But there was drug culture by prisoners and the (handwritten: “katorzhny / prison word?”)
Q. Convicts.
A. And the convicts, so it was different. Besides the Moslem culture, which is old hashish culture.
Q. And has been for a very long time. Did you find any link between either of these, either the hippie or the drug culture and any religious underground groups or mystical groups?
A. Well, a lot of hippies were interested in mystics and all kinds of religions, and a lot of them went with the different religious sects and groups afterwards or at the time of their being — hippies.
Q. What kinds of religious groups?
A. All kinds of, Christianity, zen (?) and Buddhism and all kinds of weird combinations —
Q. [laugh]
A. — between Christianity and Buddhism, without really knowing Christianity and Buddhism both. And what else?
Q. It sounds a bit like America in the end of the fifties in the beginning of the hippies.”
Episode 9.
“Q. Okay. [recorder off] Getting back to the hippies you were talking about in Moscow, how did the whole movement get started?
A. About the late sixties, quite a few people and it was the first generation of hippies and practically all of them became alcoholics now.”
Episode 10.
“А: I belong to the second generation, and in my personal opinion second generation is the best one because it was much more sophisticated than the first one, since most of the people there had some kind of… well, came from intelligentsia, and most of them had a few years of college at least, and all of them or ninety percent of them are heavy drug addicts now.”
Episode 11.
“A. We — all were social dangerous.
Q. Socially dangerous.
A. Socially dangerous, mentally ill persons, and all of us from time to time would get sent to the hospital, but what I think of all other people in Russia was we had nothing to lose anymore, and being mentally sick persons gave us the right to do a lot of things which other people would never do, and so mental hospitals were just the price which we paid for that freedom.”
Episode 12.
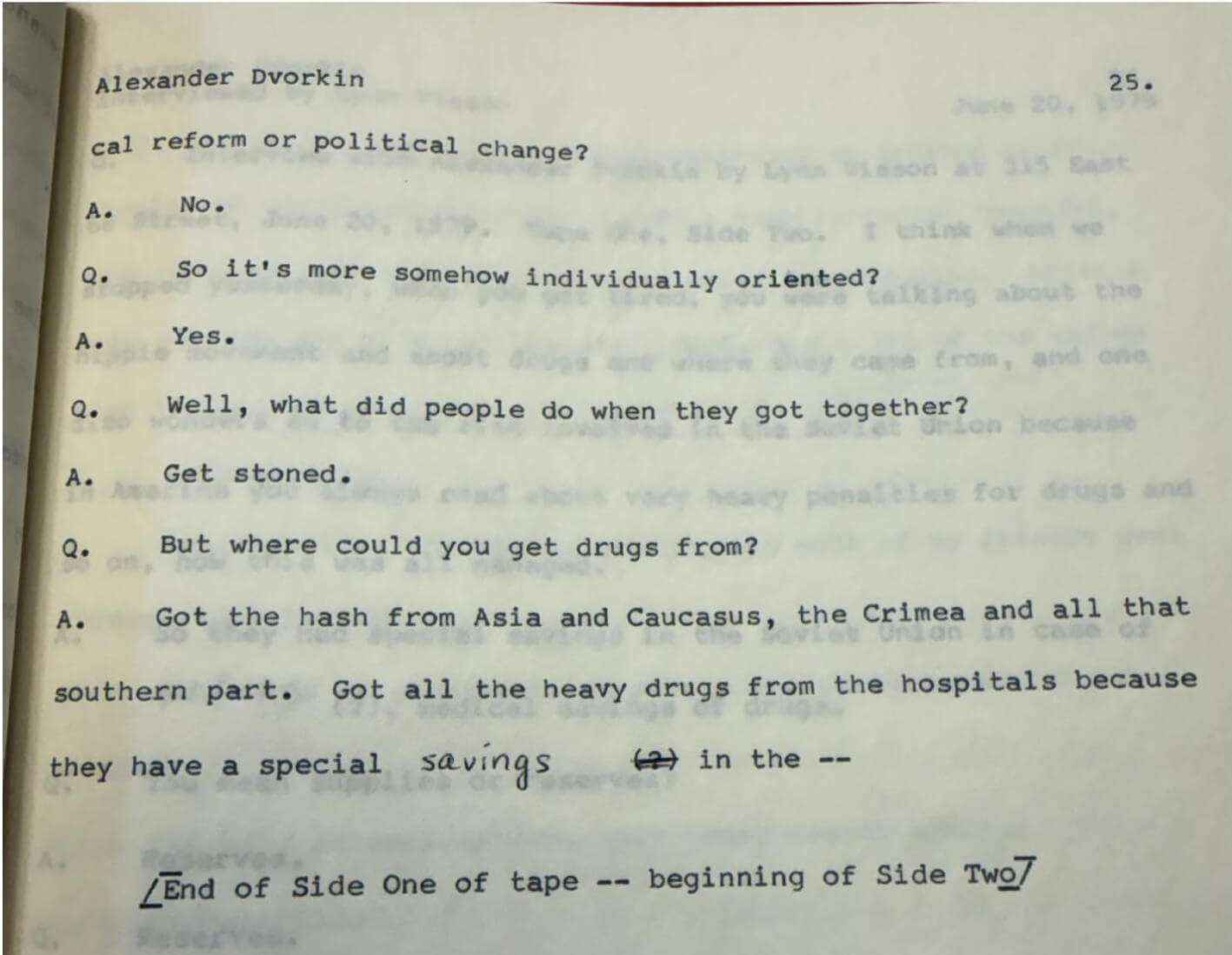
“Q: Well, what did people do when they got together?
A. Get stoned.
Q. But where could you get drugs from?
A. Got the hash from Asia and Caucasus, the Crimea and all that southern part. Got all the heavy drugs from the hospitals because they have a special savings in the –
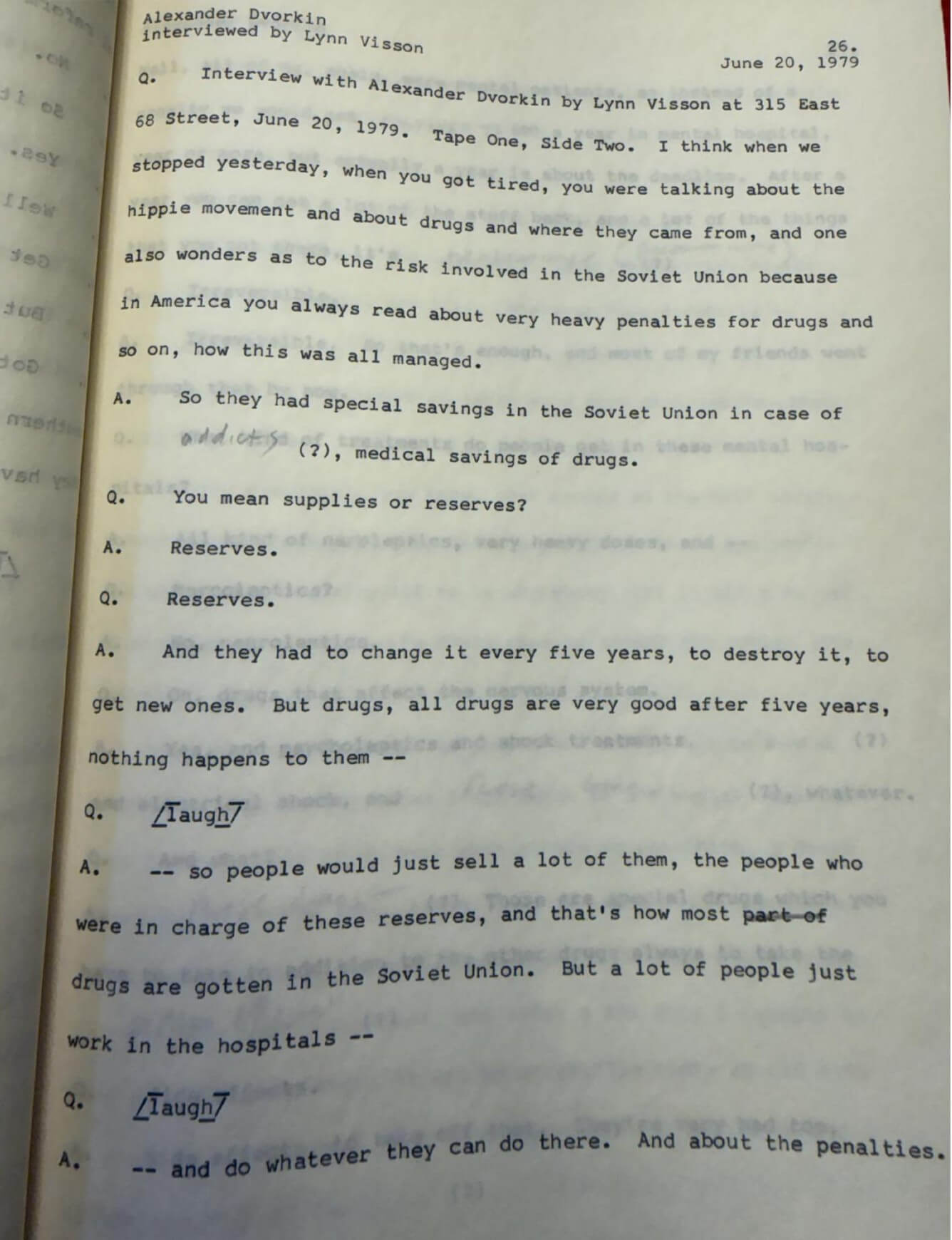
A. So they had special savings in the Soviet Union in case of addicts, medical savings of drugs.
Q. You mean supplies or reserves?
A. Reserves.
Q. Reserves.
A. And they had to change it every five years, to destroy it, to get new ones. But drugs, all drugs are very good after five years, nothing happens to them —
Q.
/laugh/
A. — so people would just sell a lot of them, the people who were in charge of these reserves, and that’s how most part of drugs are gotten in the Soviet Union. But a lot of people just work in the hospitals —
Q.
/laugh/
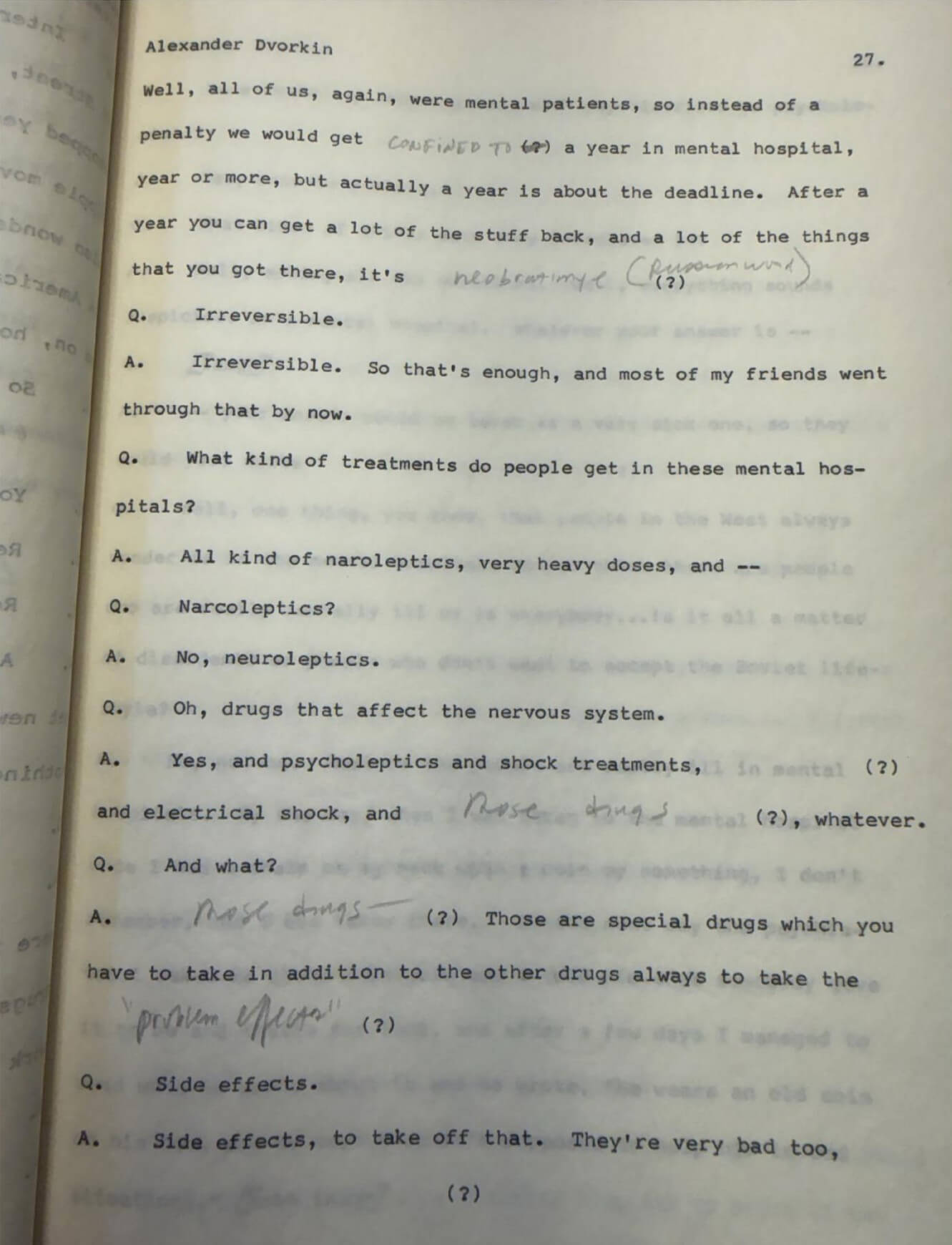
A. — and do whatever they can do there. And about the penalties. Well, all of us, again, were mental patients, so instead of a penalty we would get confined to a year in mental hospital, year or more, but actually a year is about the deadline. After a year, you can get a lot of the stuff back, and a lot of the things that you got there, it’s neobratimye (irreversible).
Q. Irreversible.
A. Irreversible. So that’s enough, and most of my friends went through that by now.
Q. What kind of treatments do people get in these mental hospitals?
A. All kind of neuroleptics, very heavy doses, and —
Q. Narcoleptics?
A. No, neuroleptics.
Q. Oh, drugs that affect the nervous system.
A. Yes, and psycholeptics and shock treatments, ______ (?) and electrical shock, and those drugs (?) whatever.
Q. And what?
A. Those drugs. Those are special drugs which you have to take in addition to the other drugs always to take the “proproblem effects” (?) —
Q. Side effects.
A. Side effects, to take off that. They’re very bad too, (?).”
Episode 13.
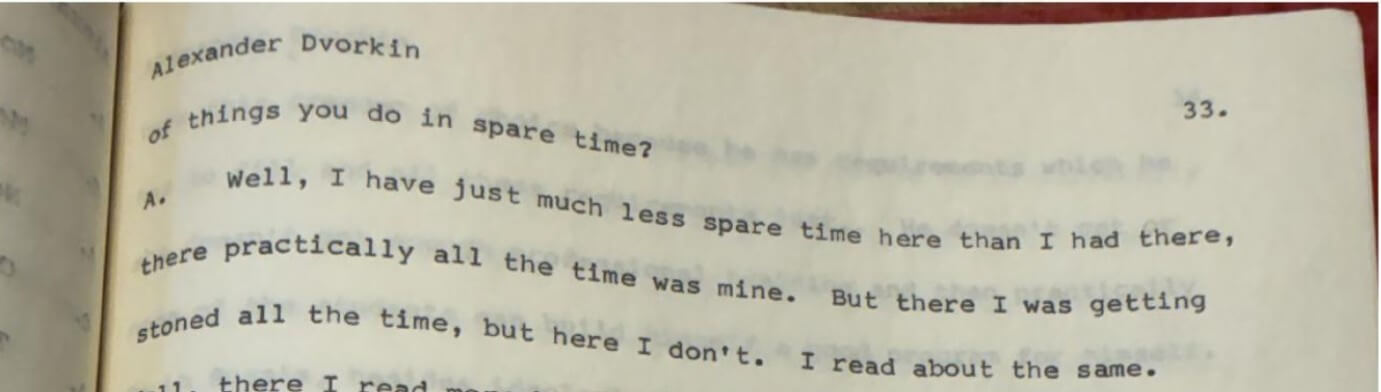
“A. Well, I have just much less spare time here than I had there; there practically all the time was mine. But there I was getting stoned all the time, but here I don’t.”
Episode 14.
“Q. Did you feel there was ever anything positive in the mental hospitals, was there any effort to help at all?
A. For the mentally ill persons?
Q. Yes.
A. Well, they were just on a very heavy drug curement.
Q. Treatment.
A. Treatment, treatment. So they were quiet under all these drugs, with all these drugs. They were just put down for all this time, and I don’t think it’s very helpful for them. It made them quiet down.
Q. Were there people you could talk to there in the mental hospital?
A. Yes. Yes, there were some very interesting patients. There were some… usually in each department there were some… I forgot the word again, katorzhnye.
Q. Convicts.
A. Convicts who were trying to get away with something, and I would talk to them.
Q. You mean by pretending to be mentally ill?
A. Yes.
Q. /laugh/ Hiding out in a mental hospital.
A. Yes. Well, because after they arrest you, if you act somehow strange, they can put you into a mental hospital to prove if you… are a mentally sick person, and if you were sick at the time of committing the crime you just get a year or more of cure in the mental hospital. So some people would prefer it. They didn’t know what would be better (?).
Q. Prefer that to prison…”
Abuse of psychoactive substances is a significant catalyst for deviant behavior. Combined with neural dysfunctions, psychopathic traits, and trauma, it reduces one’s ability to control aggression and increases the likelihood of criminal acts including serial murder. Empirical criminological data 7 show that a substantial proportion of murderers and other violent offenders actively use drugs or alcohol before committing crimes. Abuse of psychoactive substances is often accompanied by cognitive distortions, lying, a lack of empathy, and a drive for immediate gratification.
“The orderly.” Methods of learning violence. After Alexander Dvorkin was expelled from the pedagogical institute, he worked for a short period as an X-ray technician in the intensive care unit of the cardiology center at City Clinical Hospital No. 1 named after N.I. Pirogov (Moscow). However, he was fired following a conflict with the head of the facility’s administration. He then lived as a vagrant in Odesa. Later, he took a job as an orderly in the trauma intensive care unit of City Clinical Hospital No. 67 in Moscow and worked there until the summer of 1976.
For the 20-year-old Alexander Dvorkin who displayed pronounced narcissistic personality traits, an ambitious cognitive mindset of “godlikeness,” and persistent manifestations of a pathological drive for control and power over other people, the position of an orderly in a trauma intensive care unit, by his own account, seemed “appealing.” From the standpoint of psychobiographical analysis, this choice can be viewed not as accidental, but as functionally determined by his internal motivational structure and pathological needs. A trauma intensive care unit is an extreme environment involving daily encounters with human suffering, pre-death states, and technical management of vital functions through medical equipment and medications.
Given the combination of the factors listed above, including his psychiatric diagnosis, practice of polysubstance use, possession of specialized knowledge in psychopharmacology, and his motivation, Alexander Dvorkin’s professional presence in the intensive care unit created conditions for the development and escalation of his criminal inclinations. In such an environment, the subject had access to:
- high-potency pharmacological drugs including narcotic analgesics and sedatives;
- medical records containing data on diagnoses, health status, prognoses, and patients’ degree of vulnerability;
- direct contact with patients in critical condition with minimal external oversight (without witnesses), especially during his night shifts.
Such conditions could potentially facilitate the transformation of his pathological cognitive attitudes into criminal behavior.
This pattern finds confirmation in behavioral analysis research. John E. Douglas and Mark Olshaker note in their book “Mindhunter: Inside the FBI’s Elite Serial Crime Unit” 8 (published in Russian as “Psychological Portrait of a Killer”) that hospitals or nursing homes often served as places where, from time to time, they encountered serial killers who resorted to some “clean” means, such as a high-potency drug, preferring it to firearms or edged weapons. This satisfied serial killers’ need for covert control over the life and death of their victims. Moreover, this allowed serial killers to minimize external signs of violent intervention, helping to classify death as natural or resulting from the severity of an underlying illness. A factor helping to mask these crimes was the statistical expectation of fatalities in a hospital setting, which reduced the likelihood of criminal investigations and forensic examinations. This created conditions for serial killers to continue their criminal activity over extended periods of time.
In criminal psychology, this type of serial killer is referred to as a “healthcare serial killer,” while in popular literature, they are known as “angels of death.” As a rule, such an individual works as a physician, medical worker, or caregiver. They often hold a position that allows them to make decisions about terminating or continuing patients’ lives and use their knowledge to kill their victims. This type of serial killer deliberately inflicts harm and suffering on their victims. They kill patients or people under their care who suffer from incurable diseases. However, it’s important to note that their motivational structure is rarely limited exclusively to terminally ill patients: in a number of documented cases, criminal behavior extends to individuals with a favorable prognosis (healthy or easily treatable people), which indicates the dominance of controlling or sadistic motives over pseudo-altruistic ones. Injection is the most common method of administration, but it is not universal: cases have been recorded involving other methods (overdosing oral medications, altering medical equipment parameters, etc.).
In the American journal “Prosecutor,” Volume: 38 Issue 1, dated January-February 2004, an article by Karin H. Cather (2004) ‘Serial Killers, Hidden Murders: The Prosecution of Health Care Professionals Who Kill Patients” 9 presents case studies from a number of U.S. jurisdictions to show how prosecutors and investigators have successfully met the challenges of cases in which healthcare workers intentionally killed their patients:
“What makes this class of offense so difficult to detect and prosecute is that perpetrators target victims who are severely ill, even terminally ill, who cannot speak for themselves. Such patients are vulnerable to death from natural causes and to healthcare professionals who can intentionally inject lethal doses of therapeutic substances, or even essentially toxic substances, in the presence of eyewitnesses. Often there is no autopsy. End-stage Alzheimer’s patients, cancer patients, comatose persons, or the elderly and ill thus become targets for murderers in the healthcare professions.
Even if such crimes can be detected, proving them requires extensive medical evidence and winning a battle of the experts, which may include a ‘Daubert’ challenge to the admissibility of the evidence. In one of the cases described in this article, murders of two elderly nursing home patients were suspected because of the suspicious timing and circumstances of their deaths, as well as several admissions made to coworkers by the defendant. The case was driven by expert witnesses who clashed over the relative significance of extremely high postmortem morphine levels in a cancer-ridden nursing home patient. In another case, a serial murderer was detected due to a ‘spike’ in the death rate at a county hospital after the defendant was hired.”
Many documented cases indicate that healthcare serial killers 10 exhibit behavioral characteristics consistent with the organized type of serial killer: crime planning, maintaining outward control over the situation, an ability to conceal illegal activity for extended periods, etc. These killers are typically intelligent and know how to carefully and skillfully hide their crimes, using as cover the fact that deaths in hospitals are not uncommon.
There are several motivational configurations characteristic of subjects of this type:
— Controlling / sadistic motive: implementation of a need for power and control over a victim’s vital functions, when the killer exploits his position; deriving sadistic gratification from observing suffering or manifestations of patient vulnerability; in some cases, a belief in one’s own right to determine the fate of others (“I can do this,” “I’m easing the patient’s pain,” “I’m relieving suffering”);
— Pseudo-altruistic motive (“mercy killing”): when a perpetrator is convinced that he is relieving a victim of “unbearable suffering” or believes that the victim “cannot be helped anymore.” It is noteworthy that this belief may be delusional in nature or serve as a rationalization for deviant needs rather than reflecting an objective clinical picture;
— “Hero syndrome”: creation of an artificial crisis situation (e.g., by administering lethal doses of drugs that provoke deterioration in a patient’s condition), followed by the imitation of rescue measures in order to obtain social approval, recognition of professional merit, or satisfaction of narcissistic needs.
An example of a medical serial killer is Donald Harvey, an orderly convicted of serial murder. In his MasterClass guide “John Douglas Teaches How to Think Like an FBI Profiler,” 11 Douglas notes: “Donald Harvey killed up to 87 people (he was only convicted of 37 murders) over 17 years while working as an orderly and nurse’s assistant at hospitals in both Kentucky and Ohio. Though he expanded to murder outside of healthcare facilities, he typically killed in the hospitals that employed him, since he could exercise maximum control without drawing attention. That said, his nickname came from coworkers who noted, without suspicion, the number of deaths under his care. Harvey suffocated some patients, poisoned others, and even altered the settings on life-preserving devices. In 1987, police finally discovered Harvey after an autopsy of one patient revealed the presence of cyanide. He maintained that his many murders were acts of mercy for the dying.”
In their book “Mindhunter: Inside the FBI’s Elite Serial Crime Unit,” John Douglas and Mark Olshaker 8 note:
“As part of the psychobiographical analysis, it is advisable to consider retrospective data concerning Alexander Dvorkin’s professional experience as an orderly, as well as his cognitive patterns and attitudes (stable socio-psychological dispositions of his personality). Particular attention should be paid to the distorted system of beliefs, emotional reactions, and behavioral tendencies associated with the phenomenon of death. An analysis of autobiographical narratives makes it possible to reconstruct the process by which his notions of the boundary between life and death were formed, as well as to identify the relationship between the professional environment, personality traits, and deviant motivational patterns. ”
Episode 1: Alexander Dvorkin’s 1979 interview for the project “Recent Soviet Immigrants in America.” 4
“Q. You mentioned you also worked as an orderly.
A. Yes, but it was when I was in Moscow. Usually I worked during the winter since in winter I had to live in Moscow because it was just hard to bum around there. So then I had to work, so I did in winter as an orderly, as X-ray technician. I did it twice.
Q. Did you like that kind of work?
A. Yes. I’m really fascinated with medicine, but I’m really bad at physics and chemistry. I even thought of some kind of medical studies, but I don’t know chemistry or physics at all. But I studied a little medicine by myself.”
Episode 2. Information about Alexander Dvorkin from the medical archive:
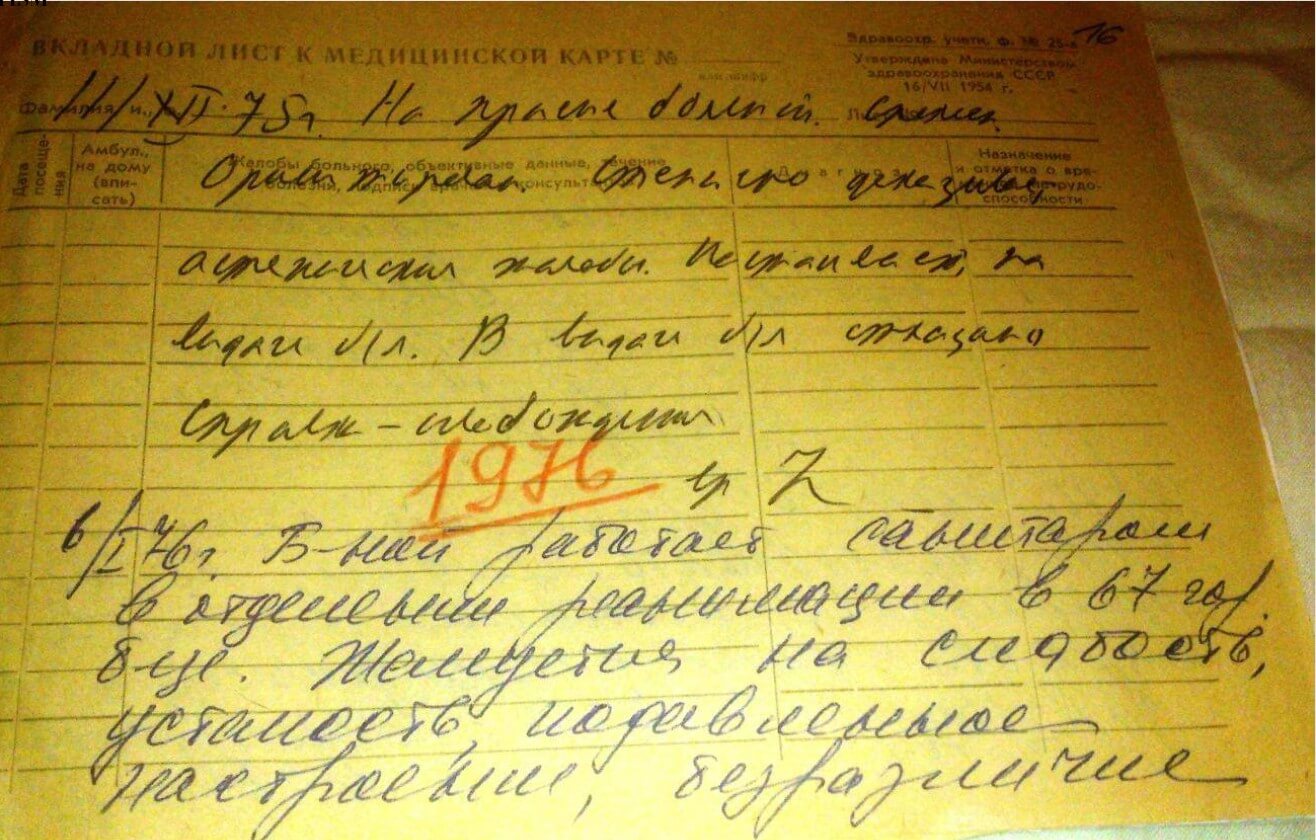
January 6, 1976. The patient works as an orderly in the intensive care unit at City Hospital No. 67. Complains of weakness, fatigue, depressed mood, and indifference to everything. He did not report to work today. He is eccentric, wears a beard and long hair.
Treatment: amitriptyline, 1/2 pill, 3 times a day.
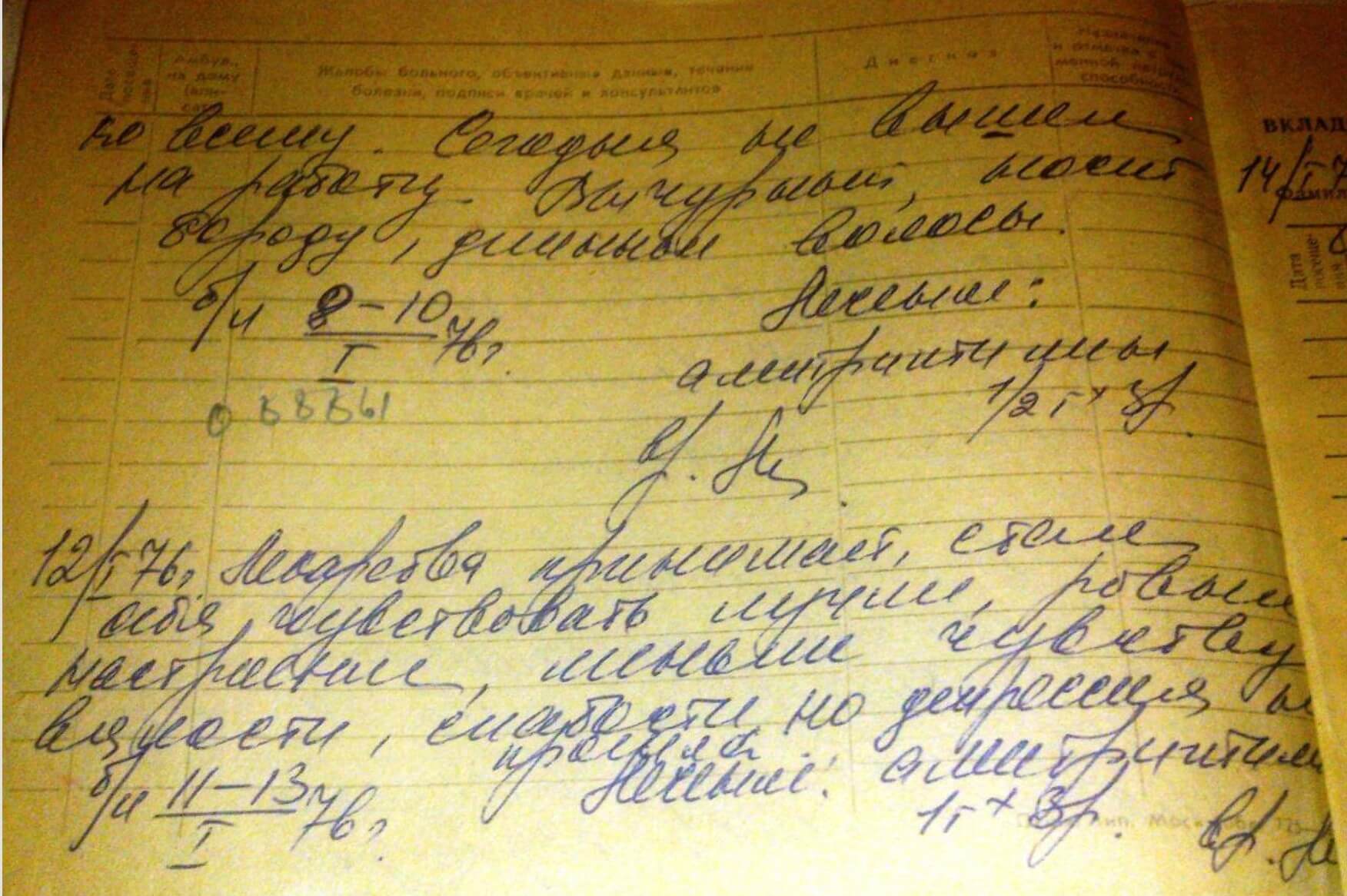
January 12, 1976.
He takes medications; began to feel better. His mood is more stable. He feels less lethargy and weakness, but depression has not passed.
Treatment: amitriptyline 1 pill, 3 times a day.
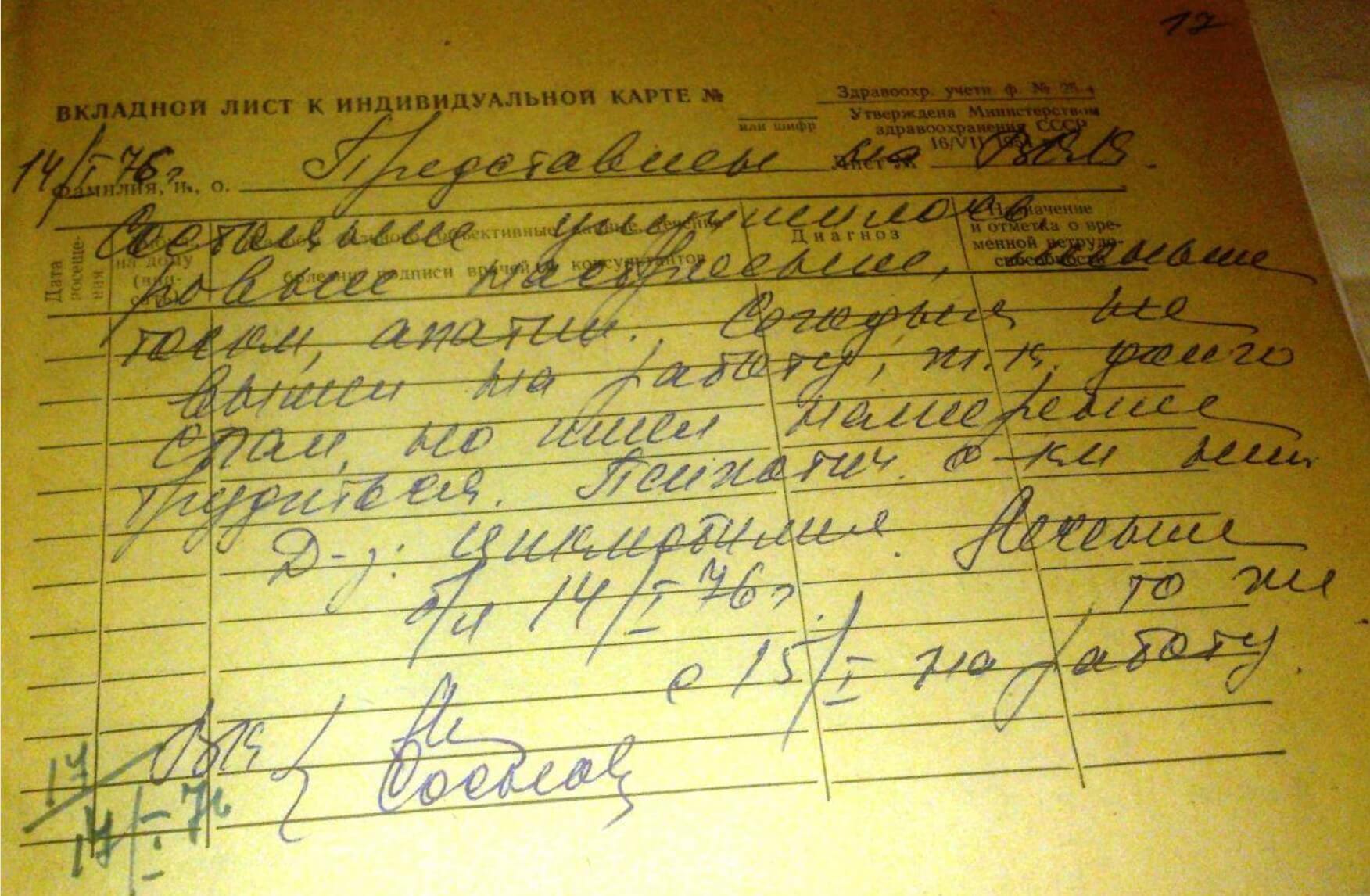
January 14, 1976. Introduced to the Military-Industrial Commission
His condition has improved, mood is more stable, less melancholy and apathy. He did not report to work today because he slept for a long time, but intended to work. No psychotic symptoms.
Diagnosis: Cyclothymia.
Treatment: unchanged
Sick leave Jan. 14, 1976; return to work Jan. 15.
Source: https://actfiles.org/alexander-dvorkins-medical-files-full-archive/
Episode 3. Excerpt from Alexander Dvorkin’s book “Teachers and Lessons. Memories, Stories, Reflections” 12:
“Naturally, being permanently expelled from the university only led Alexander to become even more actively involved in the ‘hippie’ movement.
Then, until the summer of 1976, Dvorkin worked as an orderly in the trauma intensive care unit of a hospital in Khoroshevka where his colleague was, incidentally, Evgeny Margulis, the bass guitarist for the band Mashina Vremeni [“Time Machine”]. How many tragedies and sufferings the young hippie encountered there! Nevertheless, he loved his job, and he did his best to ease the plight of the patients in the intensive care unit and provide them with at least some comfort, even before their death. Working as an orderly — a position at the very bottom of the social ladder — meant he didn’t have to lie or ‘play games’ that everyone else in Soviet society played.”
Episode 4. In his book “My America,” 5 Alexander Dvorkin shares his impressions of the course “Liturgy of Death” which he attended during his stay in the US. It was taught by Professor Alexander Schmemann, a priest. According to Dvorkin, it turned out to be “incredibly interesting” (the reasons for his interest in the topic of this lecture and the lecturer himself will be discussed in subsequent sections of our study). In this context, Alexander Dvorkin writes in his autobiographical book:
“Death has been pushed out of life; a person lives as if it does not exist, and nothing should remind him of it. Even when it is already near, everything is done so that the patient doesn’t know he is dying until the very last moment. He is constantly reassured: ‘You’re fine, there’s nothing serious, you look great, you just have a minor ailment that will soon pass. Take another medicine, and everything will be fine.’ Dying is moved within hospital walls, where a person living their last days is loaded with drugs, tranquilizers, and antidepressants — anything to keep them from being fully aware, throwing tantrums, or acting out unpredictably, so that they are not tormented by fears and may pass away into another world in a semi-conscious state. Thus, the main event of life, the final transition, takes place in a sterile, impersonal hospital setting, surrounded by orderlies, doctors, and nurses, far from home, family, and loved ones, far from any awareness of the importance of what is happening.”
Episode 5. Excerpt from Alexander Dvorkin’s book “My America” 5:
“What was I to do?
By that time, I was working as an orderly in the trauma intensive care unit of City Hospital No. 67, not far from my then home in Khoroshevka. I got the job immediately after returning from a hitchhiking trip to Odesa. The work was very demanding, but it brought me satisfaction, since I saw I was helping people in the most helpless state and thereby doing something useful. Unlike the cardiac clinic where my contact with patients was episodic (I took an X-ray and wheeled away), here I was with patients constantly. People came to us severely injured, after accidents and disasters. I tried to perform my simple duties not out of obligation, but out of conscience: I gave the patients a bedpan and a urinal, changed their beds, put pillows under them, brought them food and drink. I even learned how to give injections and, according to the patients, did it well: they often asked that I be the one to give them their shots. .”
“My partner in the unit turned out to be Yevgeny (Zhenya) Margulis, a bass guitarist from the very Mashina Vremeni (Russian ‘Time Machine’), which was gradually moving into a leading position among Moscow bands. At that time, like all the very best of them, it played English music. Zhenya and I transferred patients onto gurneys and wheeled them to surgery, then back again. We happily wheeled patients who were getting better upstairs to the medical or surgical ward, while those who had died were covered with a sheet and taken downstairs to the morgue. I remember crying when I encountered the first death of one of our patients. Although later, like most medical workers, my soul became calloused, I still felt deeply affected by each of the very frequent deaths in our unit. ”
“In my free time, I traveled several times to nearby cities: Leningrad and Kyiv, where I stayed with familiar ‘longhairs.’ If something didn’t work out, I could always spend a night or two in the stairwell. Few people dared to go hitchhiking in winter, so I adapted to riding trains without a ticket: because of the cold, ticket inspectors usually stood in the carriage, near their compartment, so you could go in and immediately jump into the rear buffer of the next carriage, pretending to be a passenger who had gone out for a smoke. When the ticket inspection was over, all that remained was to go to the reserved-seat carriage and quietly take a free seat. At worst, the upper luggage rack would do.”
These episodes from Alexander Dvorkin’s autobiography are a valuable source for psychobiographical and behavioral analysis, allowing us to reconstruct the deep psychological mechanisms underlying his self-presentation and motivational structure. The retrospective text demonstrates a high degree of narrative self-presentation. It serves as a tool for post-factum legitimization of past experiences. This is not simply a recollection arising three decades later, but a conscious construction of a personal narrative. Dvorkin creates an image of himself as an “enlightened” existential observer. This narrative structure serves not so much as a memory as a mechanism for post-factum rationalization and cognitive justification of his own actions. This pattern corresponds to the forms of narrative defense described in the literature for individuals with pronounced traits of grandiose narcissism and a tendency toward moral dissociation.
This is a typical technique described in the history of criminology, used by serial killers with a high level of intellectual reflection and moral dissociation: they rarely deny their actions outright, but reinterpret them within a philosophical, existential, or pseudo-moral system in which they present themselves not as criminals, but as “enlighteners,” “liberators,” or “witnesses to the truth.” Justifying themselves, many serial killers avoid direct statements such as “I killed,” preferring instead to say things like, “Society lies about death, but I knew the truth.” This kind of narrative allowed them to maintain a positive self-image by compensating for the cognitive dissonance between their own actions and social norms, and even to elevate their experiences, transforming violence into a form of “existential testimony.”
These and other episodes from Alexander Dvorkin’s autobiography reveal a complex duality of his inner world, demonstrating a pronounced dissociation between the image of a “humanistic person” presented in self-presentation and the real motivation of his behavior. The phrase that he “loved his job” and “tried to ease the patients’ fate” at first glance is perceived as a manifestation of altruism. However, in the context of his entire psychobiography, it takes on a different meaning. Here, a classic mechanism of moral dissociation is evident: splitting of the “good self” (the caring orderly) and the “dark self” (the controller of death). This is indicated by a number of latent yet significant details obvious to specialists in behavioral analysis, which allow for a deeper understanding of his personality, motivational frameworks, and cognitive strategies of self-description.
For example, Alexander Dvorkin’s phrases such as “very frequent deaths in our unit” and “I even learned how to give injections” testify to his violation of professional and ethical boundaries during his work as an orderly. In the Soviet healthcare system, an orderly (junior medical staff) had no right to administer injections — this fell exclusively within the competence of nurses and physicians. Alexander Dvorkin’s assertion that he “learned how to give injections” and that patients “asked that it be him” may point to the following aspects of his behavioral and motivational structure:
- Conscious violation of professional and institutional norms, which aligns with the previously described stance of “rebellion against the system” and a striving for personal autonomy;
- Desire to expand the scope of control over another person: an injection is not merely a technical procedure, but an act of direct physical intervention into a patient’s body, associated with pain, vulnerability, trust, and potential danger. For an individual with a pathological interest in power over life and death, such an act becomes a perfect means of obtaining a sense of control under the cover of care and assistance;
- A need for social approval and recognition: his mention that patients “asked that it be him” indicates a striving for external validation. This reinforces not only a sense of power, but also forms positive feedback that is extremely significant for a personality with pronounced traits of grandiose narcissism.
Notably, Dvorkin doesn’t conceal these episodes. On the contrary, he includes them in the narrative as evidence of personal autonomy and independence from institutional norms. This indicates that he takes pride in his ability to exist outside the established system, and this attitude extends to his behavior in the medical institution as well, where he “played by his own rules” (in particular, administering injections despite an official ban). Thus, the episode with injections isn’t just a mundane detail, but a behavioral marker of using the medical role as a cover to satisfy pathological needs. It also demonstrates Alexander Dvorkin’s inclination toward self-education and experimentation — traits previously noted in the context of his knowledge of psychopharmacology.
Another example — the assertion that the subject “felt deeply affected by each of the very frequent deaths” — appears as a rhetorical device aimed at creating the image of a “compassionate person.” However, in the context of his existential confrontation, narcissistic and psychopathic personality traits underlying the motivational structure (including the complex of “godlikeness” and “rebellion against God”), death for him is not a tragedy, but rather a field for exercising power and control. For him, patients were not simply suffering people, but bearers of death, so dealing with them required a certain ritual. His criticism of hospital practices more closely resembles disappointment over death being deprived of its awareness and significance: “Dying is moved within hospital walls, where a person living their last days is loaded with drugs, tranquilizers, and antidepressants — anything to keep them from being fully aware, throwing tantrums, or acting out unpredictably, so that they are not tormented by fears and may pass away into another world in a semi-conscious state.” 5 This is reminiscent of an executioner’s attitude toward the condemned. His understanding of “comfort before death” may have included not only the real alleviation of physical suffering, but also the psychological preparation of a patient for transition, possibly even for a transition under his control.
The subject’s described interest in death as an object of control fits the pattern characteristic of serial killers with a pronounced sadistic component and a need for domination. Empirical studies 13 demonstrate that such offenders do not perceive death as an abstract category, but strive for its instrumentalization, transforming it into a means of demonstrating power over their victim. The key motive is a need to control the dying process, including manipulation of a victim’s emotional state in the pre-death period. Such behavior reflects manifestations of grandiose narcissism with elements of sadism 14:
an offender seeks to occupy the position of an absolute controller of life and death, which serves to satisfy the need to confirm his own omnipotence. The demand for a victim’s “conscious participation” in the act of dying corresponds to the phenomenon described in the literature as “playing with the victim” (victim torture and psychological manipulation), where the offender prolongs the victim’s agony in order to derive pleasure from observing fear and helplessness. He wants the victim to understand what is happening, to be aware of their fate, and possibly even to enter into a pre-death dialogue with him. Such patterns reflect cognitive distortions characteristic of individuals with antisocial and sadistic personality traits.
Thus, Alexander Dvorkin’s statements become not a “justification,” but a key to understanding his inner world, for which death was evidently not an end, but a field for manifestation of his own complex of “godlikeness.” His text is less an expression of compassion than an aesthetic-ontological claim about the quality of death. In all likelihood, his “care” for patients was part of a ritual of power rather than altruism. His criticism of the hospital system may point to a projection of his own desire to control death as a meaningful, conscious act. This is typical of killers with a high level of narcissism and intellectualization of violence: they want their act to be noticed, recognized, and understood — even if the understanding belongs only to themselves.
Empirical studies show that medical serial killers systematically use professional legitimacy to mask their crimes. Medical institutions where they obtained employment provided them with specific knowledge and skills, access to resources, and anonymity necessary to commit murders without immediate detection. Daily observation of how physicians make decisions about saving lives or withholding treatment, how they use various drugs to maintain vital functions, became for potential killers a valuable source of information, including that about methods of administering medications, their effects on the body, side effects, and, most importantly, the possibility of using them as a means to accelerate death.
At the beginning of their criminal careers, serial killers learned what previously existed only in their fantasies: they learned how to minimize traces, give the process the appearance of a natural cause of death, and how to deceive the surveillance system. This was a decisive stage in their transformation from an individual with pathological desires into a perpetrator of murder — the one who wanted not merely to see death, but to control it consciously, personally, and without intermediaries. Such practice provided them not just with technical preparation for the use of pharmacological substances for non-clinical purposes, but also with rehearsal of role behavior associated with managing extreme states of the human organism. Thus, working in healthcare institutions became for them a “school of violence” and a place to acquire skills for implementing a pathological need to control life and death under the cover of social usefulness. Subsequent events in their lives became catalysts for escalation and modification of their murder methodology.
Correlation with the relational factor, subfactor “Ways of learning violence” in the SIR model:
SF5: Ways of learning violence. From what we can deduce, a human being is not born a serial killer, but, over years, learns the use of violence to satisfy his needs (identity, sexual, personal gratification, omnipotence) and ways of learning are always a question of interaction with one or more negative patterns taken as reference points.
Read the full report.
Source:
1. Rita Z Goldstein, Nora D Volkow «Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications»
https://pmc.ncbi.nlm.nih.gov/articles/PMC3462342/#:~:text=Abstract
https://nida.nih.gov
2. M. Brower, B. Price «Neuropsychiatry of frontal lobe dysfunction in violent and criminal behaviour: a critical review»
https://pmc.ncbi.nlm.nih.gov/articles/PMC1737651/#:~:text=violent%20and%20criminal%20behaviour%20suggest,impulsive%20subtype%20of%20aggressive%20behaviour
3. Book “Kalalatsy” by Arkady Rovner — Moscow: “New Time” International Association of People of Culture, PSK Timan, 1990.
4. A 1979 interview with Alexander Dvorkin for the project “Recent Soviet Immigrants in America.”
Interviewer: Lynn Visson (June 19–20, 1979). William E. Wiener Oral History Library of the American Jewish Committee. New York Public Library (NYPL) Research Libraries.
https://archive.org/details/alexander-dvorkin-interview-june-19-1979/page/n5/mode/2up
5. Alexander Dvorkin. “My America” (2013)
https://fb2.top/moya-amerika-813075
6. Elinore F. McCance-Katz, Lynn Sullivan, Srikanth Nallani: «Drug Interactions of Clinical Importance among the Opioids, Methadone and Buprenorphine, and other Frequently Prescribed Medications: A Review»
https://pmc.ncbi.nlm.nih.gov/articles/PMC3334287/#:~:text=
7. R M Yarvis «Patterns of Substance Abuse and Intoxication Among Murderers», 1994
https://www.ojp.gov/ncjrs/virtual-library/abstracts/patterns-substance-abuse-and-intoxication-among-murderers#:~:text=manslaughter%20who%20were%20referred%20for,important%20etiological%20contributor%20to%20some
8. John E. Douglas and Mark Olshaker note in their book “Mindhunter: Inside the FBI’s Elite Serial Crime Unit”.
9. Karin H. Cather (2004) ‘Serial Killers, Hidden Murders: The Prosecution of Health Care Professionals Who Kill Patients”. Prosecutor Volume: 38 Issue: 1 Dated: January-February 2004
https://www.ojp.gov/ncjrs/virtual-library/abstracts/serial-killers-hidden-murders-prosecution-health-care-professionals
10. Angel of mercy (criminology) https://en.wikipedia.org/wiki/Angel_of_mercy_(criminology)
11. «John Douglas Teaches How to Think Like an FBI Profiler»
12. Alexander Dvorkin’s book “Teachers and Lessons. Memories, Stories, Reflections” (2008)
https://www.labirint.ru/books/240384/
13. Ressler, R. K., Burgess, A. W., & Douglas, J. E. (1988). Sexual homicide: Patterns and motives. Lexington Books/D. C. Heath and Com.
https://psycnet.apa.org/record/1988-97582-000
14. J. Reid Meloy «Nature and Dynamics of Sexual Homicide: An Integrative Review». Journal Aggression and Violent Behavior Volume: 5 Issue: 1 Dated: January-February 2000 Pages: 1-22
https://www.ojp.gov/ncjrs/virtual-library/abstracts/nature-and-dynamics-sexual-homicide-integrative-review





